What Does Excess Fluid Around the Baby Mean
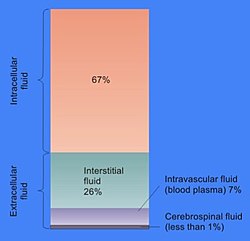
In prison cell biological science, extracellular fluid (ECF) denotes all body fluid outside the cells of any multicellular organism. Total body water in healthy adults is nigh sixty% (range 45 to 75%) of total torso weight;[ citation needed ] women and the obese typically have a lower percentage than lean men.[1] Extracellular fluid makes up about one-third of body fluid, the remaining two-thirds is intracellular fluid inside cells.[two] The main component of the extracellular fluid is the interstitial fluid that surrounds cells.
Extracellular fluid is the internal environment of all multicellular animals, and in those animals with a claret circulatory arrangement, a proportion of this fluid is blood plasma.[3] Plasma and interstitial fluid are the ii components that make up at least 97% of the ECF. Lymph makes up a small percentage of the interstitial fluid.[iv] The remaining small portion of the ECF includes the transcellular fluid (about 2.5%). The ECF tin also be seen equally having two components – plasma and lymph as a delivery system, and interstitial fluid for water and solute exchange with the cells.[five]
The extracellular fluid, in particular the interstitial fluid, constitutes the trunk'southward internal environment that bathes all of the cells in the torso. The ECF composition is therefore crucial for their normal functions, and is maintained by a number of homeostatic mechanisms involving negative feedback. Homeostasis regulates, among others, the pH, sodium, potassium, and calcium concentrations in the ECF. The volume of body fluid, blood glucose, oxygen, and carbon dioxide levels are likewise tightly homeostatically maintained.
The volume of extracellular fluid in a young adult male of seventy kg (154 lbs) is 20% of body weight – about fourteen litres. Eleven litres is interstitial fluid and the remaining three litres is plasma.[6]
Components [edit]
The chief component of the extracellular fluid (ECF) is the interstitial fluid, or tissue fluid, which surrounds the cells in the body. The other major component of the ECF is the intravascular fluid of the circulatory system called blood plasma. The remaining small per centum of ECF includes the transcellular fluid. These constituents are often called fluid compartments. The volume of extracellular fluid in a immature adult male of lxx kg, is twenty% of body weight – virtually 14 litres.
Interstitial fluid [edit]
The interstitial fluid is essentially comparable to plasma. The interstitial fluid and plasma make upward almost 97% of the ECF, and a small percentage of this is lymph.
Interstitial fluid is the torso fluid between blood vessels and cells,[vii] containing nutrients from capillaries by diffusion and holding waste products discharged out by cells due to metabolism.[8] 11 litres of the ECF is interstitial fluid and the remaining iii litres is plasma.[half-dozen] Plasma and interstitial fluid are very similar because h2o, ions, and small solutes are continuously exchanged betwixt them across the walls of capillaries, through pores and capillary clefts.
Interstitial fluid consists of a h2o solvent containing sugars, salts, fatty acids, amino acids, coenzymes, hormones, neurotransmitters, white blood cells and prison cell waste material-products. This solution accounts for 26% of the water in the homo body. The composition of interstitial fluid depends upon the exchanges between the cells in the biological tissue and the blood.[x] This means that tissue fluid has a different composition in dissimilar tissues and in dissimilar areas of the trunk.
The plasma that filters through the blood capillaries into the interstitial fluid does not contain red claret cells or platelets as they are too big to laissez passer through simply can contain some white blood cells to help the allowed organisation.
In one case the extracellular fluid collects into small vessels (lymph capillaries) it is considered to be lymph, and the vessels that bear it back to the claret are called the lymphatic vessels. The lymphatic organization returns protein and excess interstitial fluid to the apportionment.
The ionic composition of the interstitial fluid and blood plasma vary due to the Gibbs–Donnan effect. This causes a slight difference in the concentration of cations and anions between the 2 fluid compartments.
Transcellular fluid [edit]
Transcellular fluid is formed from the transport activities of cells, and is the smallest component of extracellular fluid. These fluids are contained inside epithelial lined spaces. Examples of this fluid are cerebrospinal fluid, aqueous humor in the eye, serous fluid in the serous membranes lining body cavities, perilymph and endolymph in the inner ear, and articulation fluid.[1] [11] Due to the varying locations of transcellular fluid, the limerick changes dramatically. Some of the electrolytes present in the transcellular fluid are sodium ions, chloride ions, and bicarbonate ions.
Part [edit]

Cell membrane details between extracellular and intracellular fluid

Sodium-potassium pump and the diffusion between extracellular fluid and intracellular fluid
The extracellular fluid provides the medium for the substitution of substances between the ECF and the cells, and this can accept identify through dissolving, mixing and transporting in the fluid medium.[12] Substances in the ECF include dissolved gases, nutrients, and electrolytes, all needed to maintain life.[13] The ECF also contains materials secreted from cells in soluble form, but which quickly coalesces into fibres (east.thou. collagen, reticular, and elastic fibres) or precipitates out into a solid or semisolid course (e.k. proteoglycans which grade the bulk of cartilage, and the components of bone). These and many other substances occur, peculiarly in association with various proteoglycans to grade the extracellular matrix or the "filler" substance between the cells throughout the body.[14] These substances occur in the extracellular space, and are therefore all bathed or soaked in ECF, without existence part of the ECF.
Oxygenation [edit]
One of the primary roles of extracellular fluid is to facilitate the exchange of molecular oxygen from blood to tissue cells and for carbon dioxide, COii, produced in cell mitochondria, back to the blood. Since carbon dioxide is about twenty times more soluble in water than oxygen, information technology can relatively easily diffuse in the aqueous fluid between cells and blood.[15]
However, hydrophobic molecular oxygen has very poor water solubility and prefers hydrophobic lipid crystalline structures.[16] [17] As a event of this, plasma lipoproteins can carry significantly more than O2 than in the surrounding aqueous medium.[xviii] [19]
If hemoglobin in erythrocytes is the principal transporter of oxygen in the blood, plasma lipoproteins may be its merely carrier in the ECF.
The oxygen-carrying chapters of lipoproteins, OCCL, reduces in ageing or in inflammation. This results in changes of ECF functions, reduction of tissue Otwo supply and contributes to development of tissue hypoxia. These changes in lipoproteins are caused by oxidative or inflammatory harm.[20]
Regulation [edit]
The internal surroundings is stabilised in the procedure of homeostasis. Complex homeostatic mechanisms operate to regulate and keep the composition of the ECF stable. Individual cells can also regulate their internal limerick by diverse mechanisms.[21]

Differences in the concentrations of ions giving the membrane potential.
There is a pregnant divergence betwixt the concentrations of sodium and potassium ions within and outside the cell. The concentration of sodium ions is considerably higher in the extracellular fluid than in the intracellular fluid.[22] The converse is true of the potassium ion concentrations inside and outside the prison cell. These differences cause all cell membranes to be electrically charged, with the positive accuse on the outside of the cells and the negative accuse on the inside. In a resting neuron (non conducting an impulse) the membrane potential is known equally the resting potential, and between the two sides of the membrane is about -70 mV.[23]
This potential is created by sodium-potassium pumps in the cell membrane, which pump sodium ions out of the cell, into the ECF, in return for potassium ions which enter the cell from the ECF. The maintenance of this difference in the concentration of ions between the inside of the cell and the outside, is critical to keep normal cell volumes stable, and as well to enable some cells to generate action potentials.[24]
In several cell types voltage-gated ion channels in the cell membrane can be temporarily opened under specific circumstances for a few microseconds at a fourth dimension. This allows a brief inflow of sodium ions into the cell (driven in past the sodium ion concentration gradient that exists betwixt the exterior and inside of the cell). This causes the prison cell membrane to temporarily depolarize (lose its electric charge) forming the basis of action potentials.
The sodium ions in the ECF also play an important role in the movement of water from i body compartment to the other. When tears are secreted, or saliva is formed, sodium ions are pumped from the ECF into the ducts in which these fluids are formed and nerveless. The h2o content of these solutions results from the fact water follows the sodium ions (and accompanying anions) osmotically.[25] [26] The same principle applies to the formation of many other torso fluids.
Calcium ions have a keen propensity to bind to proteins.[27] This changes the distribution of electrical charges on the protein, with the consequence that the 3D (or tertiary) construction of the protein is contradistinct.[28] [29] The normal shape, and therefore part of very many of the extracellular proteins, as well as the extracellular portions of the cell membrane proteins is dependent on a very precise ionized calcium concentration in the ECF. The proteins that are particularly sensitive to changes in the ECF ionized calcium concentration are several of the clotting factors in the blood plasma, which are functionless in the absenteeism of calcium ions, but get fully functional on the add-on of the correct concentration of calcium salts.[22] [27] The voltage gated sodium ion channels in the cell membranes of nerves and muscle have an fifty-fifty greater sensitivity to changes in the ECF ionized calcium concentration.[30] Relatively small decreases in the plasma ionized calcium levels (hypocalcemia) cause these channels to leak sodium into the nerve cells or axons, making them hyper-excitable, thus causing spontaneous muscle spasms (tetany) and paraesthesia (the sensation of "pins and needles") of the extremities and round the mouth.[28] [30] [31] When the plasma ionized calcium rises above normal (hypercalcemia) more than calcium is bound to these sodium channels having the contrary issue, causing lethargy, muscle weakness, anorexia, constipation and labile emotions.[31] [32]
The third structure of proteins is besides affected by the pH of the bathing solution. In addition, the pH of the ECF affects the proportion of the total amount of calcium in the plasma which occurs in the free, or ionized form, equally opposed to the fraction that is bound to poly peptide and phosphate ions. A change in the pH of the ECF therefore alters the ionized calcium concentration of the ECF. Since the pH of the ECF is directly dependent on the partial pressure of carbon dioxide in the ECF, hyperventilation, which lowers the partial pressure of carbon dioxide in the ECF, produces symptoms that are almost duplicate from low plasma ionized calcium concentrations.[28]
The extracellular fluid is constantly "stirred" by the circulatory organization, which ensures that the watery environment which bathes the body's cells is virtually identical throughout the body. This means that nutrients can be secreted into the ECF in one place (east.g. the gut, liver, or fat cells) and will, within about a infinitesimal, exist evenly distributed throughout the torso. Hormones are similarly chop-chop and evenly spread to every cell in the body, regardless of where they are secreted into the blood. Oxygen taken up past the lungs from the alveolar air is also evenly distributed at the correct partial pressure to all the cells of the body. Waste products are too uniformly spread to the whole of the ECF, and are removed from this general circulation at specific points (or organs), once once more ensuring that there is mostly no localized accumulation of unwanted compounds or excesses of otherwise essential substances (e.g. sodium ions, or any of the other constituents of the ECF). The only pregnant exception to this general principle is the plasma in the veins, where the concentrations of dissolved substances in individual veins differ, to varying degrees, from those in the residue of the ECF. However, this plasma is confined within the waterproof walls of the venous tubes, and therefore does non affect the interstitial fluid in which the body's cells live. When the blood from all the veins in the torso mixes in the heart and lungs, the differing compositions abolish out (e.g. acidic claret from active muscles is neutralized past the element of group i blood homeostatically produced by the kidneys). From the left atrium onward, to every organ in the body, the normal, homeostatically regulated values of all of the ECF's components are therefore restored.
Interaction between the blood plasma, interstitial fluid and lymph [edit]

Germination of interstitial fluid from blood.

Diagram showing the germination of lymph from interstitial fluid (labeled hither as "Tissue fluid"). The tissue fluid is entering the blind ends of lymph capillaries (shown as deep greenish arrows)
The arterial blood plasma, interstitial fluid and lymph interact at the level of the blood capillaries. The capillaries are permeable and water can move freely in and out. At the arteriolar terminate of the capillary the blood force per unit area is greater than the hydrostatic pressure in the tissues.[33] [22] Water will therefore seep out of the capillary into the interstitial fluid. The pores through which this h2o moves are large enough to allow all the smaller molecules (up to the size of small proteins such as insulin) to move freely through the capillary wall also. This means that their concentrations beyond the capillary wall equalize, and therefore have no osmotic issue (considering the osmotic pressure acquired past these minor molecules and ions – chosen the crystalloid osmotic pressure to distinguish it from the osmotic event of the larger molecules that cannot move across the capillary membrane – is the same on both sides of capillary wall).[33] [22]
The movement of water out of the capillary at the arteriolar finish causes the concentration of the substances that cannot cross the capillary wall to increase as the blood moves to the venular end of the capillary. The most important substances that are bars to the capillary tube are plasma albumin, the plasma globulins and fibrinogen. They, and especially the plasma albumin, because of its molecular abundance in the plasma, are responsible for the so-chosen "oncotic" or "colloid" osmotic force per unit area which draws h2o dorsum into the capillary, specially at the venular stop.[33]
The net event of all of these processes is that water moves out of and back into the capillary, while the crystalloid substances in the capillary and interstitial fluids equilibrate. Since the capillary fluid is constantly and apace renewed by the period of the blood, its composition dominates the equilibrium concentration that is achieved in the capillary bed. This ensures that the watery environment of the body's cells is always close to their ideal environs (set by the body'due south homeostats).
A modest proportion of the solution that leaks out of the capillaries is not drawn dorsum into the capillary by the colloid osmotic forces. This amounts to between 2-4 liters per day for the body as a whole. This water is collected by the lymphatic organisation and is ultimately discharged into the left subclavian vein, where it mixes with the venous blood coming from the left arm, on its way to the heart.[22] The lymph flows through lymph capillaries to lymph nodes where bacteria and tissue debris are removed from the lymph, while various types of white blood cells (mainly lymphocytes) are added to the fluid. In addition the lymph which drains the small intestine contains fat droplets called chylomicrons after the ingestion of a fatty meal.[27] This lymph is called chyle which has a milky appearance, and imparts the proper noun lacteals (referring to the milky appearance of their contents) to the lymph vessels of the minor intestine.[34]
Extracellular fluid may be mechanically guided in this circulation past the vesicles between other structures. Collectively this forms the interstitium, which may be considered a newly identified biological structure in the torso.[35] However, there is some debate over whether the interstitium is an organ.[36]
Electrolytic constituents [edit]
Main cations:[37]
- Sodium (Na+) 136–146 mM
- Potassium (K+) three.viii–5.0 mM
- Calcium (Catwo+) 1.0–1.4 mM
Main anions:[37]
- Chloride (Cl−) 103–112 mM
- Bicarbonate (HCO3 −) 22–28 mM
- Phosphate (HPO4 two−) 0.viii-1.4 mM
[38]
Encounter likewise [edit]
- Effective circulating book (ECV)
- Fluid compartments
References [edit]
- ^ a b "Fluid Physiology: 2.1 Fluid Compartments". world wide web.anaesthesiamcq.com . Retrieved 2019-xi-28 .
- ^ Tortora G (1987). Principles of beefcake and physiology (5th ed.). New York, NY: Harper and Row. p. 693. ISBN978-0-06-350729-6.
- ^ Hillis D (2012). Principles of life. Sunderland, MA: Sinauer Associates. p. 589. ISBN978-one-4292-5721-3.
- ^ Pocock Grand, Richards CD (2006). Human physiology : the basis of medicine (third ed.). Oxford: Oxford University Press. p. 548. ISBN978-0-19-856878-0.
- ^ Canavan A, Arant BS (Oct 2009). "Diagnosis and direction of dehydration in children" (PDF). American Family Physician. fourscore (7): 692–six. PMID 19817339.
- ^ a b Hall J (2011). Guyton and Hall textbook of medical physiology (12th ed.). Philadelphia, Pa.: Saunders/Elsevier. pp. 286–287. ISBN978-1-4160-4574-viii.
- ^ Wiig, Helge; Swartz, Tune A. (2012). "Interstitial Fluid and Lymph Formation and Transport: Physiological Regulation and Roles in Inflammation and Cancer". Physiological Reviews. American Physiological Guild. 92 (iii): 1005–1060. doi:ten.1152/physrev.00037.2011. ISSN 0031-9333. PMID 22811424. S2CID 11394172.
- ^ "Definition of interstitial fluid". world wide web.cancer.gov. 2011-02-02. Retrieved 2022-03-08 .
- ^ Widmaier, Eric P., Hershel Raff, Kevin T. Strang, and Arthur J. Vander. "Body Fluid Compartments." Vander's Man Physiology: The Mechanisms of Torso Function. 14th ed. New York: McGraw-Hill, 2016. 400-401. Print.
- ^ Constanzo LS (2014). Physiology (fifth ed.). Elsevier Saunders. p. 264. ISBN9781455708475.
- ^ Tortora G (1987). Principles of anatomy and physiology (5th ed. Harper international ed.). New York: Harper & Row. pp. 61–62. ISBN978-0-06-046669-5.
- ^ Tortora G (1987). Principles of beefcake and physiology (5th ed. Harper international ed.). New York: Harper & Row. p. 17. ISBN978-0-06-046669-5.
- ^ Voet D, Voet J, Pratt C (2016). Fundamentals of Biochemistry: Life at the Molecular Level. Hoboken, New Bailiwick of jersey: John Wiley & Sons. p. 235. ISBN978-1-118-91840-one.
- ^
- ^ Bačič, Thousand.; Walczak, T.; Demsar, F.; Swartz, H. M. (October 1988). "Electron spin resonance imaging of tissues with lipid-rich areas". Magnetic Resonance in Medicine. viii (2): 209–219. doi:10.1002/mrm.1910080211. PMID 2850439. S2CID 41810978.
- ^ Windrem, David A.; Plachy, William Z. (August 1980). "The diffusion-solubility of oxygen in lipid bilayers". Biochimica et Biophysica Acta (BBA) - Biomembranes. 600 (3): 655–665. doi:10.1016/0005-2736(80)90469-one. PMID 6250601.
- ^ Petyaev, I. M.; Vuylsteke, A.; Bethune, D. Westward.; Hunt, J. V. (1998-01-01). "Plasma Oxygen during Cardiopulmonary Bypass: A Comparison of Blood Oxygen Levels with Oxygen Nowadays in Plasma Lipid". Clinical Scientific discipline. 94 (1): 35–41. doi:10.1042/cs0940035. ISSN 0143-5221. PMID 9505864.
- ^ Jackson, Thou. J. (1998-01-01). "Plasma Oxygen during Cardiopulmonary Featherbed". Clinical Scientific discipline. 94 (1): 1. doi:x.1042/cs0940001. ISSN 0143-5221. PMID 9505858.
- ^ Petyaev, Ivan K.; Hunt, James Five. (April 1997). "Micellar dispatch of oxygen-dependent reactions and its potential use in the study of human low density lipoprotein". Biochimica et Biophysica Acta (BBA) - Lipids and Lipid Metabolism. 1345 (3): 293–305. doi:10.1016/S0005-2760(97)00005-2. PMID 9150249.
- ^ Pocock K, Richards CD (2006). Human being physiology : the footing of medicine (3rd ed.). Oxford: Oxford University Printing. p. three. ISBN978-0-19-856878-0.
- ^ a b c d e Tortora 1000 (1987). Principles of anatomy and physiology (5th ed.). New York: Harper & Row, International. pp. 40, 49–50, 61, 268–274, 449–453, 456, 494–496, 530–552, 693–700. ISBN978-0-06-046669-5.
- ^ Tortora G (1987). Principles of Anatomy and Physiology . p. 269. ISBN978-0-06-046669-5.
- ^ Tortora Grand (2011). Principles of anatomy and physiology (13th ed.). Hoboken, Northward.J.: Wiley. pp. 73–74. ISBN978-0-470-64608-3.
- ^ Tortora Grand, Anagnostakos Due north (1987). Principles of anatomy and physiology (5th ed.). New York, NY: Harper and Row. pp. 34, 621, 693–694. ISBN978-0-06-350729-6.
- ^ "Information". pcwww.liv.ac.uk.
- ^ a b c Stryer L (1995). Biochemistry (Fourth ed.). New York: Due west.H. Freeman and Company. pp. 255–256, 347–348, 697–698. ISBN0-7167-2009-4.
- ^ a b c Macefield G, Burke D (Feb 1991). "Paraesthesiae and tetany induced by voluntary hyperventilation. Increased excitability of human cutaneous and motor axons". Brain. 114 ( Pt 1B) (1): 527–40. doi:10.1093/brain/114.1.527. PMID 2004255.
- ^ Stryer L (1995). Biochemistry (4th ed.). New York: W.H. Freeman and Company. pp. 347, 348. ISBN978-0-7167-2009-6.
- ^ a b Armstrong CM, Cota G (March 1999). "Calcium block of Na+ channels and its upshot on closing charge per unit". Proceedings of the National Academy of Sciences of the Us of America. 96 (vii): 4154–vii. Bibcode:1999PNAS...96.4154A. doi:10.1073/pnas.96.7.4154. PMC22436. PMID 10097179.
- ^ a b Harrison TR. Principles of Internal Medicine (third ed.). New York: McGraw-Hill Volume Company. pp. 170, 571–579.
- ^ Waters M (2009). "Hypercalcemia". InnovAiT. 2 (12): 698–701. doi:10.1093/innovait/inp143.
- ^ a b c Hall J (2011). Guyton and Hall textbook of medical physiology (12th ed.). Philadelphia, Pa.: Saunders/Elsevier. pp. 177–181. ISBN978-1-4160-4574-eight.
- ^ Williams PL, Warwick R, Dyson M, Bannister LH (1989). Gray's Beefcake (Thirty-seventh ed.). Edinburgh: Churchill Livingstone. p. 821. ISBN0443-041776.
- ^ Rettner R (27 March 2018). "Meet Your Interstitium, a Newfound "Organ"". Scientific American . Retrieved 28 March 2018.
- ^ "Is the Interstitium Really a New Organ?". The Scientist.
- ^ a b Diem Grand, Lentner C (1970). "Blood – Inorganic substances". in: Scientific Tables (Seventh ed.). Basle, Switzerland: CIBA-GEIGY Ltd. pp. 561–568.
- ^ Guyton & Hall Textbook of Medical Physiology (page five)
External links [edit]
- Britannica.com
- Biology-online.org
Source: https://en.wikipedia.org/wiki/Extracellular_fluid
0 Response to "What Does Excess Fluid Around the Baby Mean"
Enviar um comentário